Welcome to Pregnancy
Laura Whisler, M.D. Janna Chibry, M.D. Maggie Woods, M.D. Ashley Robbins, M.D. Katie Marney, D.O.
Congratulations on this amazing journey of pregnancy! Whether this is your first pregnancy or your last or somewhere in between, we are here to help you through it! We are so very excited that we get to experience this pregnancy with you and your family!
This note is VERY important for you to read! It will answer many questions you may have or that may come up. We want to work with you to help make you and your baby as healthy as possible during your pregnancy and delivery.
We strongly advise that you connect to our patient portal so you can stay up to date on your results and health information. It is an easy way to contact a nurse or for us to contact you, if needed. Check your email regularly regarding your care at College Hill OB/GYN. This being said, in between appointments, most communication will be by phone. Please make sure you keep us up to date with your phone number and other contact information. In an emergency always call 911.

VERY IMPORTANT
Portal Set-Up Instructions
After clicking the button below, click ‘Create an Account’ and follow the form’s instructions to create an account and a password.
It’s very easy and an important part of your care!
Your Appointment Schedule
- You will have an appointment with your doctor every 4-6 weeks before you are 30 weeks along.
- Once you are 30 weeks, you will see your doctor every 2-3 weeks.
- Starting at 35-36 weeks, you will see your doctor on a weekly basis.
Pregnancy Financial Policy
- Every patient will receive information regarding your insurance coverage for this pregnancy prior to your appointment with detailed information regarding an estimate of the patient responsibility. If you have not received this information prior to your appointment, please contact the College Hill Billing Department as payment may be required at your initial appointment.
- Should payment be due, you will be required to sign an agreement to pay a set amount throughout your pregnancy to ensure the ESTIMATE balance is paid prior to delivery.
Common Pregnancy Symptoms
First Trimester
- Nausea is normal, but if extreme, you need to let our office know. We can prescribe you medications to help or if severe you may need IV hydration.
- Lower abdominal pain or cramping is normal. Please notify us if the pain is severe or if there is associated bleeding. Tylenol and/or Benadryl can be used, as needed.
- Heartburn – Tums are ok to use as needed.
Second & Third Trimester
- Headaches are one of the most common symptoms in the 2nd trimester. Do NOT use Ibuprofen for your headaches unless I advise otherwise. Tylenol is safe. Drink plenty of fluids and make sure your protein and calorie intake are high enough. Also, if you recently stopped caffeine, this could be a reason for your headache.
- Nausea at this point may be associated with GERD – try Pepcid and if no relief, let me know.
- Lower abdominal pain is usually normal and usually associated with the ligaments (round ligament pain). Use Tylenol to help. If it is affecting you a lot, we can refer you for physical therapy. If it is severe, notify us immediately or go to labor and delivery.
- It is NOT normal to feel isolated contractions (regular abdominal tightness, downward pressure and cramping that grows stronger, longer and closer together) before 37 weeks. If they occur, use Tylenol and Benadryl, drink 1 liter of water and rest. If they persist after 2-3 hours go to labor and delivery.
- It IS normal to have Braxton Hicks contractions (Self-resolving, irregular, infrequent abdominal tightness, downward pressure, and mild cramping) throughout your pregnancy starting at 20 weeks.
- Shortness of breath – if it is NOT associated with chest pain, a cough, or sustained fast heart rate, it is related to normal body function during pregnancy.
- Low Back Pain – a prenatal belt will help along with exercise. You can also use Tylenol for the pain. It is an effect from the curvature of the spine in pregnancy. If you have higher back pain under your rib cage, that could be associated with kidney stones or a kidney infection. Please notify the nurse or me if that is the case so your urine can be tested. Also, notify us if you develop a fever.
- Leg Swelling – we check your blood pressure every time you come in. If it is normal, your leg swelling is likely associated with how the blood flows through your body when you are pregnant. Elevating your feet and compression stockings are helpful in that case.
Important Information to Tell Your Doctor
- Please provide a list of all medications and dosages that you take.
- Heart Defects – Please inform me if you, your significant other or a first degree relative (parents, siblings, other children) of you are your significant other has or has had a heart defect of any type.
- Health problems
- Hypertension – Outside of pregnancy have you ever been told or been treated for high blood pressure. Let us know if so.
- Diabetes – currently or a history of gestational diabetes.
- Thyroid disease
- Any other heart problem
- Eating disorder
- Blood Clots or Stroke
- Diseases associated with bleeding.
- Lupus or any other autoimmune disorder
- Seizures
- Asthma
- Cancer
- Drug or alcohol use during this pregnancy
- Any other health conditions.
- If you are bleeding, leaking clear fluid or having contractions.
- Are you electing surgical sterilization post-delivery or are you interesting in birth control post delivery? Please discuss with your physician prior to delivery.
Previous Pregnancy Complications
- Gestational Diabetes
- High Blood Pressure associated with pregnancy.
- Preterm labor and/or delivery
- Prior pregnancy complicated by a birth defect.
- Growth restriction
- Delivery complications
- Cesarean sections, including the reason for your C-section.
- Any other pregnancy or delivery complications
Safe Medications During Pregnancy
Pain Medications
Tylenol/Acetaminophen (preferred), Ibuprofen up until 26 weeks along
Decongestants & Expectorants
Benadryl (Diphenhydramine), Pseudoephedrine, Guaifenesin (Mucinex), Dextromethorphan (Robitussin), Cough Drops, Vicks VapoRub
Antihistamines
Chlorpheniramine (Chlor-Trimeton), Benadryl (Diphenhydramine), Zyrtec
Diarrhea
Kao pectate (Antidiarrheal of choice), Imodium
DO NOT use Pepto Bismol or Lomotil
Constipation
Psyllium (Metamucil), Polycarbophil (Fiber-Lax), Methylcellulose (Citrucel), Colace, Dulcolax, Milk of Magnesia
Hemorrhoids
Anusol, Preparation H, Tucks
Antacids
Maalox, Mylicon, Tums, Simethicone (Mylanta), Cimetidine (Tagamet), Famotidine (Pepcid), Nexium
Yeast Infections
Monistat (Miconazole or Ticonazole), Butoconazole (Femstat)
Insomnia
Benadryl, Unisom, Doxylamine
Itching
Hydrocortisone
Nausea/Vomiting
Vitamin b6 25mg every 8 hrs, doxylamine 25mg every 8 hrs, ginger chews, peppermint
Your Diet During Pregnancy
- During pregnancy, eating healthy does not mean eating a lot! During the first trimester, you really don’t need extra calories. During the second trimester increase calories by about 300 calories a day and 400 in the third trimester.
- Eat healthy portions of fruits and vegetables, protein, complex carbohydrates and milk or dairy products.
- It is helpful to eat 3 small meals and 3 light high protein snack to reduce headaches, lightheadedness, and weakness.
- You should be on a prenatal vitamin with 400 mcg of folic acid. Your prenatal vitamins should also have iron in it. Many of the over-the-counter prenatal vitamins do not have iron, so double-check that yours does. If it does not, pick up a different one, or let your nurse or doctor know, and we can prescribe one for one.
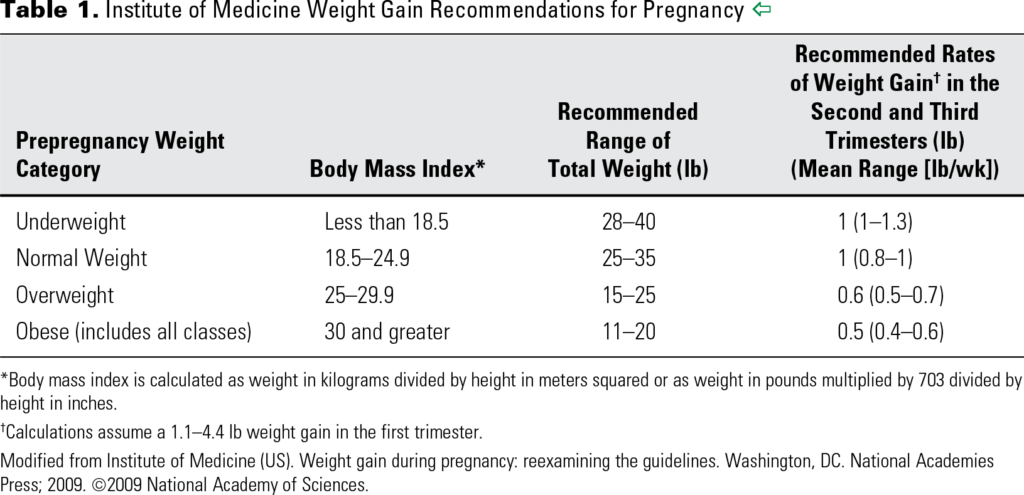
Weight Gain
- Do not be surprised if you lose some weight at the beginning. This is common as long as it isn’t a large percentage of your weight, your baby will not be affected.
Unsafe Foods
- Raw seafood
- Soft cheese
- Unpasteurized milk/cheese
- Mexican cheese
- Pate
- Raw or undercooked meat and poultry
- Microwave all lunch meats
- Alcohol (at any amount)
Fish Intake
- High levels of mercury have been associated with fetal brain development.
- Limit fish to 1 serving every week.
- Choose fish low in mercury (salmon, shrimp, polluck, tuna (light canned), tilapia, catfish, and cod)
- Avoid fish high in mercury (tilefish from the Gulf of Mexico, shark, swordfish, king mackerel)
Exercise in Pregnancy
- It is encouraged that you exercise regularly in pregnancy unless your doctor tells you otherwise. 30 minutes, at least 5 days a week is what is recommended by ACOG.
- It is okay to begin an exercise program during pregnancy, but do not put yourself in a position where you could fall, get hurt or cannot control your breathing. Also, do not strain while lifting weights. Everyone is different, but once you hit 20 weeks along, you should not lift more than 40 pounds.
- You should NOT exercise if you have a restrictive heart or lung condition, if you have cerclage, history of preterm labor, persistent bleeding, placenta previa, premature labor, ruptured membranes, preeclampsia, severe anemia, fetal growth restriction.
Smoking in Pregnancy
- Smoking is associated with many pregnancy complications including growth restriction, preeclampsia, placental problems, preterm delivery and cesarean section. This is a great time to quit, and we are happy to help.
- Kansas has a helpline (KanQuit – 1 (800) 784-8669 or 1 (800) QUIT-NOW; www.kanquit.org)
Travel in Pregnancy
- In an uncomplicated pregnancy, air travel should be limited at 36 weeks. We will let you know based on risk whether air travel should be limited before then.
- Some airlines have strict rules, and you will need to contact them directly.
- If possible, limit ground travel during your lats 3 weeks of pregnancy if it is more than 2 hours away.
- Always get out of the vehicle every 2 hours to walk around if you are on long road trips before then.
Zika Virus in Pregnancy
- Everything you need to know regarding Zika in Pregnancy can be found on ACOG’s website.
- Travel Restrictions – Updated: December 19, 2016
- Pregnant women should not travel to areas where ima outbreaks are ongoing.
- Specific areas in Florida (as of June 15)
- Specific areas in Texas (as of October 29)
- Puerto Rico
- Specific areas of Southeast Asia (as of September 29)
- Pregnant women and their partners who must travel to one of these areas should strictly follow steps to prevent mosquito bites druing the trip and decrease the risk for sexual transmission.
- *Areas of local transmission within the U.S. will likely change frequently.
- Pregnant women should not travel to areas where ima outbreaks are ongoing.
- Prevention – Updated: October 18, 2016
- Avoiding exposure is best.
- When traveling to areas where Zika virus has been reported, women should take all precautions to avoid mosquito bites including the use of EPA-approved bug spray with DEET, covering exposed skin, staying in air-conditioned or screened-in areas, and treating clothing with permethrin.
- Providers should specifically communicate to pregnant women that when used as directed on the product label, EPA-registered insect repellents, particularly those with DEET and permethrin, can be used safely during pregnancy.
- These protective measures should be followed both day and night as the Aedes Aegyptus mosquito (which carries Zika virus) bites primarily during the day as well as dusk and dawn. Reapplication of insect repellant should be practiced as directed on the product label.
- Consistently and correctly using condoms during sex or abstaining from sex for the duration of the pregnancy is recommended if you have a sex partener that has traveled to or lives in an area with active Zika virus transmission.
Vaccinations
Flu Shot
ACOG recommends the flu shot in pregnancy. If you have state (Medicaid) insurance, you will be provided with a prescription to obtain your Flu shot at Walgreens, CVS or even the health department as it is NOT covered by your insurance at our office. Not only will the Flu shot help protect you baby, but the flu during pregnancy is also a lot harder on you compared to when you are not pregnant, and you are 10X more likely to die from the flu during pregnancy.
TDAP
This vaccine is recommended during the 3rd trimester. This vaccine is mostly for your baby. He / She cannot get the whooping cough vaccine until at least 2 months of life. If you get it during your pregnancy, it will help provide protection in that first 2 months, which is when babies get sick from it. All members of the household should be up to date on the TDAP, as well as including those who will provide direct care to your newborn.
COVID-19
The American College of Obstetricians and Gynecologists (ACOG) strongly recommends that all eligible persons receive the COVID-19 vaccine. This applies to patients planning to become pregnant, who are currently pregnant, and who are currently breast-feeding.
RSV
This vaccine is recommended between weeks 32-36.6 if your due date is between Sept 1 and Jan 31. The goals it to help reduce severe RSV in the 1st 6 months of life.
General Health
- Please continue your general health visits with your dentist or other specialists (neurology, pain doctor, psychiatrist, PCP, etc.) during your pregnancy.
- You can have dental work performed if general anesthesia is not used.
Laboratory Evaluations
Prenatal Labs – ordered at your 1st or 2nd visit.
- Prenatal labs include screening for HIV, Hepatitis B, Syphilis, anemia, platelets, immunity to Rubella and a urinary tract infection.
- We will also be finding out your blood type (negative blood type will be addressed later on this page) and a specific lab (antibody screen) that tests for the possibility of a undesirable reaction of your red blood cells to the baby’s red blood cells. This is rare.
- Even though you may be at low or no risk, the hospital requires that these labs be drawn and available for them and the pediatrician. Additional lab work will depend on other health-related factors.
Genetic Testing – 10-22-week Appointment
- At your initial visit you received information about genetic screening options. Your insurance does NOT always cover them, so you will want to make sure by calling them ahead of time.
- If you or your significant other have a family history of cystic fibrosis or spinal muscular atrophy or arise from Ashkenazi Jewish descent, we would strongly recommend this test.
- If you have a family history of autism, mental retardation, or early menopause I would strongly recommend screening for Fragile X.
- First Trimester screening is also an option between 12-14 weeks and requires a specialized ultrasound done at a High-Risk Maternal Fetal Medicine Consultation. It is slightly more sensitive than the Pentagon Screen and you can get information sooner in the first trimester.
- Special considerations:
- African Americans – ALL should be screened for Sickle Cell Trait and will be with your prenatal labs.
- Advanced Maternal Age (AMA; ≥ 35 years old) – you would likely qualify for Q-natal or Cell Free Fetal DNA, which is a more specific test based on your higher risk of Trisomy.
- YOU WILL NEED TO CHECK WITH YOUR INSURANCE REGARDING COVERAGE AS THIS TEST IS VERY EXPENSIVE.
24-28-week Labs
- These labs include a repeat antibody screen, anemia screen and a 1-hour Glucose Tolerance Test (GTT), which is a screen for gestational diabetes. When you have an appointment between 24 weeks and 28 weeks along, anticipate this lab work.
- DRINK ONLY WATER AND DO NOT EAT ANYTHING APPROXIMATELY 3 HOURS BEFORE THIS VISIT!!
- The test takes 1 hour of your time that day.
- You will need an early 1-hour GTT if you have a personal history of Gestational Diabetes, or your BMI is >35. Please inform your doctor if you have had Gestational Diabetes. If your early test is negative, it will be repeated at 24-28 weeks.
Group B Strep (GBS) – 35-36-week Appointment
- At your 35-36-week appointment, I will screen for GBS. It is a vaginal swab that screens for a natural bacterium (normal flora) that approximately 20% of women have. It does NOT cause discharge or any kind of symptoms/problems in you, but CAN affect your baby (sepsis, meningitis, pneumonia).
- A positive result indicates the need for antibiotics during the labor process, so that your baby can have the antibiotics in his/her blood during vaginal passage. The antibiotics do a very good job at preventing infection in your baby, we simply need to know whether you need them. It is extremely rare for your baby to be affected be GBS if you are adequately treated. Your baby’s pediatrician usually watches your baby for 48 hours in the hospital if you are GBS positive.
Ultrasounds
Ultrasound for Dating
- You may have your first ultrasound prior to your initial appointment. This ultrasound must be scheduled but will usually be done within 1-3 business days.
- This ultrasound will confirm or may even change your due date when compared to your last menstrual period. If your due date changes a nurse will call you and notify you of this change. AFTER THIS POINT, YOUR ESTIMATED DUE DATE WILL NOT EVER CHANGE, NO MATTER WHAT SUBSEQUENT ULTRASOUNDS MAY SAY!
Complete Pregnancy Ultrasound (CPS)
- You will have a CPS between 18-22 weeks (depending on Body Mass Index (BMI)). This ultrasound must be scheduled and can take 20-60 minutes. If you choose to find out the gender of your baby, you will be able to at this ultrasound. If there are abnormalities on this ultrasound, your doctor will call you to discuss this with you.
Follow-Up Ultrasounds
- ALL insurances will cover 2 ultrasounds ONLY, unless there are specific complications that can arise (IE: Gestational Diabetes, Pregnancy induced hypertension, etc.)
- Your insurance will NOT cover an ultrasound for gender reveal or a third or more ultrasound if there are no complications occurring.
Your Delivery
Delivery Site
- We deliver at Wesley Medical Center and Wesley Birth Care Center ONLY.
- Please notify our staff or your doctor of where you would like to deliver.
- Tours are available at Wesley and the Wesley Birth Care Center by calling (316) 962-3222.
- If this is your first pregnancy and your cervix is unfavorable (<3cm) the Wesley Birth Care Center does not allow for an induction, and you would need to be induced at the main hospital. However, if you are in labor, your water breaks and you’re breaks and you’re at least 37 weeks along you may present to the Birth Care Center for Evaluation.
- Certain high-risk situations disqualify you for the Birth Care Center as well (VBAC, hypertension, birth defects, etc.)
Delivery Coverage
- Our doctors have a rotating call schedule beginning at 5:00 p.m. until 7:00 a.m. every weeknight and during the weekends, so that we may have an opportunity to be at home with our families, travel and to have the opportunity to sleep or rest.
- Although it is your doctor’s absolute goal to deliver you, that may not be possible. The other doctors in the call pool are excellent and we are very confident with how they care for patients and know you are in excellent hands under their care.
- On average, nine times out of ten your doctor will be there and available for your delivery!
Delivery Birth Plans
- Many patients come to their doctor with a birth plan. Sample birth plans can be found on the internet or in your hospital packet.
- If you have specific desires during your labor and delivery, please bring them up during your last month (or sooner if desired)
- As long as the safety of you and your baby aren’t at stake, your preferences can almost always be met.
VBAC
- Vaginal birth after cesarean section is an option for patients who have had TWO prior cesarean section.
- It does have risks, but those risks are low (1%), but include the uterus breaking open during labor and need for an emergency cesarean section or a low risk of fetal brain damage.
- Indications for your previous cesarean section will help guide our decision together. For instance, women who have had a vaginal delivery before her cesarean section are excellent VBAC candidates and should highly consider it. Or women who have not ever delivered vaginally AND the indication for their cesarean section was related to lack of progression in their labor are more likely to fail a trial of labor. If you have a history of cesarean section, please notify your doctor by 28 weeks your preference.
Episiotomy
- It is not standard to perform an episiotomy during your delivery. We believe, based on experience, that lacerations tend to extend more if an episiotomy is made. Only in the instance where the baby is not tolerating the last bit of labor and we need to expedite your delivery will an episiotomy be performed. We always perform a midline episiotomy unless you have other desires. We do have patients request episiotomy and we will be happy to perform if you so desire.
Assisted Delivery (Forceps or Vacuum Delivery)
- There is indication for Forceps and Vacuum deliveries. The only alternative to these is a cesarean section. Risks are very low. We will only use these measures if it is indicated. For example, if you have been pushing for a few hours and are exhausted and desire assistance or if your baby is low in the pelvis and NOT tolerating labor (usually seen by monitoring the fetal heart rate monitor), we can expedite your delivery for the sake of your baby’s health. We would never use these tools for our own convenience!
Pain Control
- You may use IV pain control up until about 6-7cm dilation. If you were to delivery soon after receiving a dose of IV pain medication, it can reduce your baby’s efforts to breathe, so that is why we limit its use beyond that point. The IV pain medication does NOT affect your baby while you are pregnant, because you are providing him or her the nutrients they need.
- Epidural is immediately available upon request at all hospitals. There is no cervical dilation that limits your ability to get an epidural. We have had patients completely dilated get one. You just have to be able to sit still and not be pushing. The anesthesiologist will discuss the risks associated with epidural during your delivery.
- Pudendal nerve block is using local numbing medication in the vagina to block some sensation of the vulva and vagina. It will not help with painful contraction but may reduce pain for vaginal stretching.
Skin-to-Skin
- Skin-to-skin is standard at all hospitals. It has great advantages for mom and baby. There are some circumstances that immediate skin-to-skin is not possible. These include Assisted Delivery, meconium staining, or other complications. It is always my goal for your and your baby to have that time if the baby’s safety is not in jeopardy.
Delayed Cord Clamping
- The NICU doctors and pediatricians are recommending delayed cord clamping (1 minute) due to its health benefits. It is our standard practice. There are also some limitations to this which are the same limitations to skin-to-skin.
Others
- Please let your doctor know if there are any other preferences you must make your delivery as you would like it. It is such an amazing experience! Desires regarding room environment, music, guests, massage, positioning, etc. should be verbalized with the nurse taking care of you during your labor.
Contacting Us With Concerns of Labor
- If you have questions of whether you need immediate evaluation on labor and delivery, you can call our main number (316) 683-6766. After hours, this pages our on-call nurse, and she will call you once she receives your page. If you call during business hours, you will be directed to a nurse. If it is a question they cannot answer (rare), they will get in contact with your doctor or the doctor on call to help answer your question.
- If you feel concerned regarding labor, your water breaking, bleeding, reduced movement of your baby or more, do not hesitate to go into labor and delivery. The resident doctors or nurses will contact your doctor or the doctor on call directly.
- Contractions – You need to go into labor and delivery if you are having 6-10 contractions in an hour for 2 or more hours (if <37 weeks) or contractions every 3-5 minutes (if >37 weeks). Try to use 1000mg of Tylenol, 25mg of Benadryl, rest, and drink one liter of water. If they continue or get closer together or are stronger, present to labor and delivery.
- Ruptured Membranes – If your water breaks (slow constant leak or gush) go into labor and delivery immediately.
- Bleeding – Any bleeding that is like a period or that concerns you go directly to labor and delivery. Spotting after intercourse is common, but is not normal for it to be heavy.
- Reduced fetal movement – of any kind or level of concern – go to labor and delivery if after hours or call our office to be scheduled for testing. Do NOT wait until the next appointment. After 32 weeks, the baby should move 6-10 times in 2 hours. If there is any concern or a reduction from what is normal for your baby it needs to be evaluated right away.
- Do not hesitate to contact us with any other concern you may have.
Again, congratulations on your pregnancy! I am so very excited to be a part of it! I look forward to spending time with you and getting to know you and your family and eventually meeting your baby!
Take Care,
Laura Whisler
Janna Chibry
Maggie Woods
Ashley Robbins
Katie Marney




